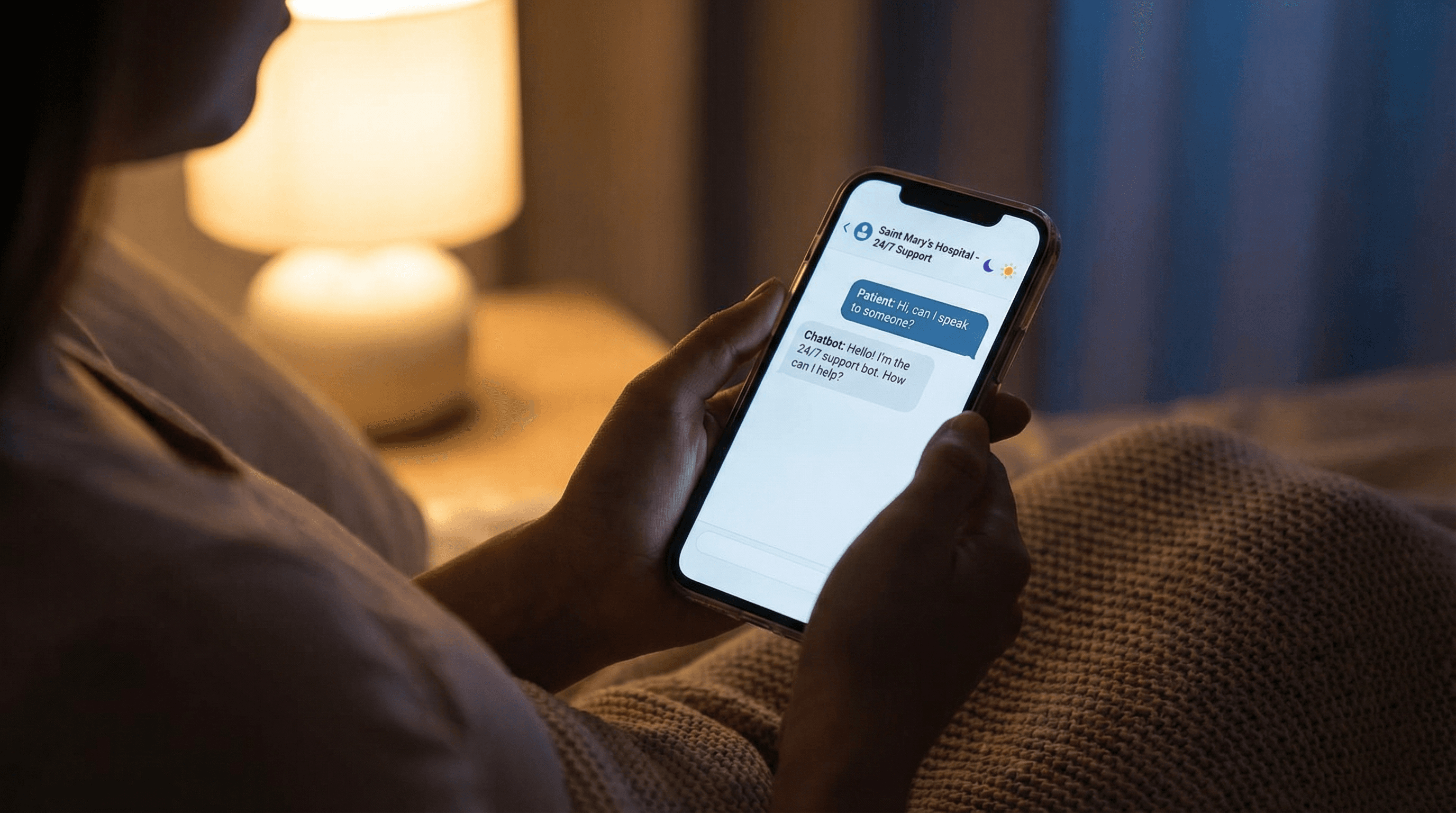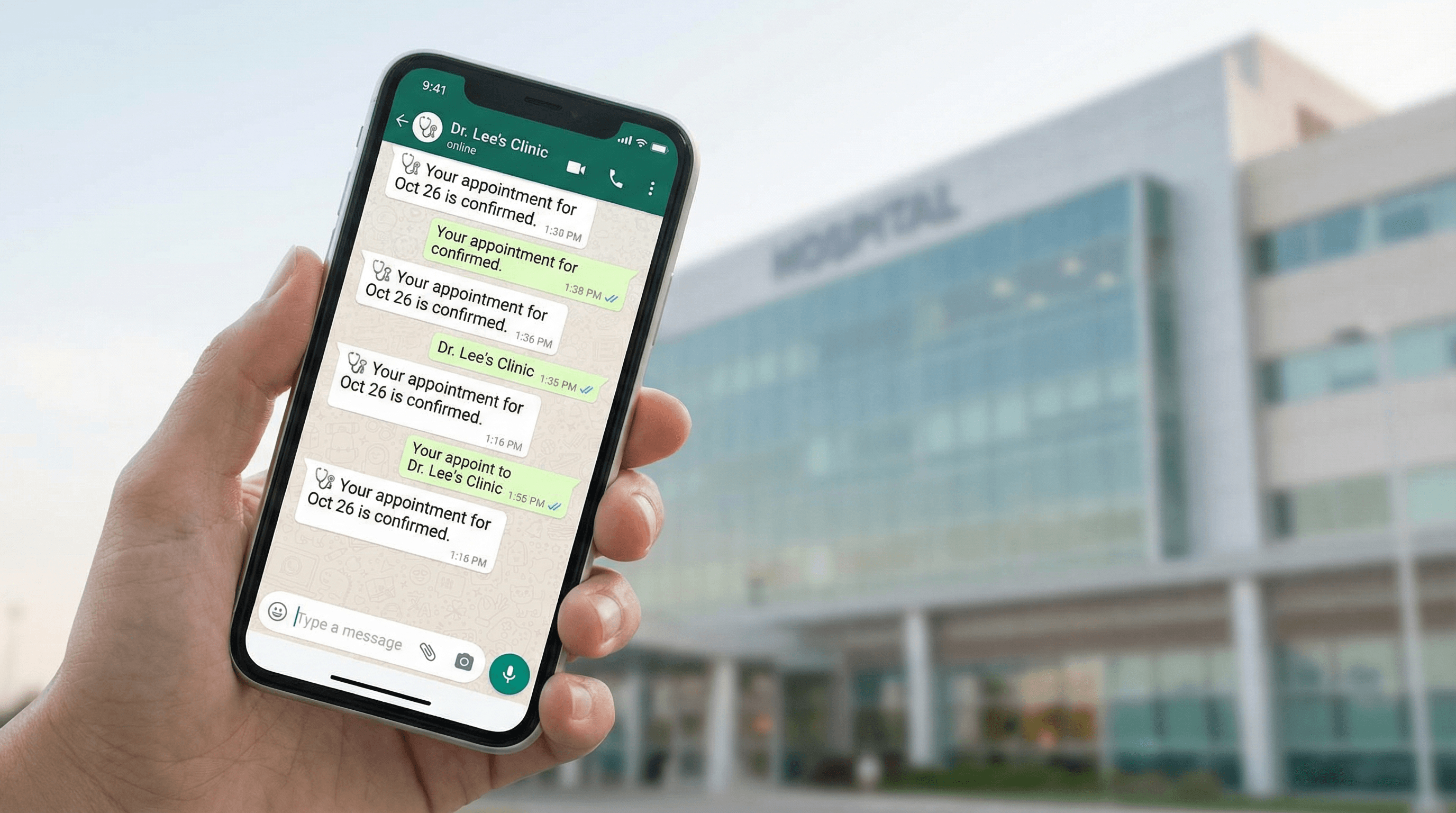
Struggling to manage patient messages on WhatsApp?
Bot MD automates WhatsApp patient enquiries for hospitals — replies in seconds, not hours.
Real hospitals. Real results.
See how hospitals in Singapore, Philippines, and Indonesia use Bot MD to automate patient engagement and recover lost revenue.
View case studies →